Main content
Setting
The case originates from a 64-bed hospital in Makeni Town, northern Sierra Leone. About 60% of Sierra Leoneans live below the poverty line. Life expectancy at birth is 58 years. The hospital has an operating theatre, pharmacy and basic diagnostic facilities. The medical staff consists of an experienced Global Health doctor, a clinical officer, and a clinical health assistant. The nearest referral hospital is in the capital city Freetown, about 5 hours’ drive from Makeni.
| Case A newborn with a large (12 x 6 centimetres) congenital mass on the left side of his chest was referred to the hospital (Figure 1). Apart from the mass, the boy was doing well. On examination, the painless mass felt soft and fluctuant, mobile from the chest wall and from the skin. Normal breathing sounds were heard over the chest on auscultation; no breathing sounds could be heard over the mass. Ultrasound examination showed fluid inside the mass. An X-ray showed a normal image of heart and lungs. It did appear however that the ribs on the left side of the chest were indented. |

Specialist advice
The Global Health doctor thought of a congenital cyst. She consulted the specialists of Consult Online for advice on diagnosis and management, in particular if performing surgical excision would be the best treatment option. The paediatricians and surgeons of Consult Online responded the next day. It was felt that lymphangioma was the most likely diagnosis. The suggestion for treatment was aspiration of the content and injecting a sclerosing agent (such as aethoxysclerol or tetracycline – if possible dissolved in lidocaine, for local pain management). Surgical excision was not recommended. The preferred timeframe for performing the procedure was when the child would be a few months old.
Follow-up
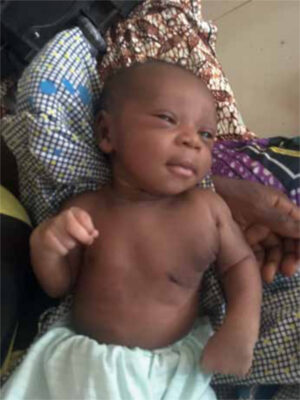
The mother required prompt treatment, since the child’s acceptance by the father depended on the treatment of the lymphangioma. Unfortunately, none of the options mentioned for sclerosing agents were available. After an extensive search, povidone iodine was found as a readily locally available sclerosing agent. At one week of age, the child was treated: aspiration of clear fluid was done and injection with povidone iodine 10%. After this, the location of the former mass was bandaged. The child developed some fever, which responded well to paracetamol and antibiotics. After a couple of weeks, the mother brought the child for check-up to the outpatient clinic: he was doing very well and and a clear reduction in size of the mass was seen. (Figure 2).
Background
The cystic variety of lymphangioma, called cystic lymphangioma or cystic hygroma, is a relatively rare benign congenital tumour of the lymphatic system. Cystic lymphangioma is the most common form of all types of lymphangiomas.[1] Cystic lymphangioma results from developmental malformation of the lymphatic system.
Clinical features
Cystic lymphangiomas can manifest anywhere in the body but usually affect the head and neck (75%), with a predilection for the left side. Approximately 20% of cystic lymphangiomas occur in the axilla, and they have also been reported to occur within the chest wall.[2,3] The usual time of presentation is at birth (>60%).[1] It presents as a painless, soft and compressible mass. Ultrasound examination of the mass shows a (multi-) cystic lesion without blood flow. Cystic lymphangioma itself is harmless and can remain asymptomatic for a long period of time, but complications may arise. Most importantly, they are prone to infection, spontaneous hemorrhage in the cyst may occur, and depending on the location and size of the cyst, respiratory distress or feeding difficulty can be a problem.[1] A minority of patients can show spontaneous partial regression of the lymphangioma, but complete spontaneous resolution is not to be expected.[1] On aspiration, cystic lymphangioma may produce milky, serous, serosanguinous or straw-coloured fluid.[1]
Treatment
Indications for treatment include the above-mentioned complications, cosmetic reasons, and interference with motor development. The ideal treatment used to be surgical excision, but this is not an easy task, with risks of possible complications (infection, bleeding, iatrogenic damage to nerves or other surrounding structures). Therefore, aspiration and injection of a sclerosing agent was recommended in this case. Povidone iodine is not the sclerosing agent of choice if other agents are available, since povidone iodine resorption could lead to hypothyroidism.[4] Fortunately, the child involved in our case showed no signs of hypothyroidism on follow-up.
References
- Mirza B, Ijaz L, Saleem M, Sharif M, Sheikh A. Cystic hygroma: an overview. Cutan Aesthet Surg. 2010;3(3):139-144.
- Eren S, Avci A. Giant cystic lymphangioma in the thoracic wall in a newborn. Asian Cardiovasc Thorac Ann. 2009;17(6):659.
- Yildirim E, Dural K, Kaplan T, Sakinci U. Cystic lymphangioma: report of two atypical cases. Interact Cardiovasc Thorac Surg. 2004;3(1):63.
- Kovacikova L, Kunovsky P, Lakomy M, et al. Thyroid hormone status after cardiac surgery in infants with delayed sternal closure and continued use of cutaneous povidone-iodine. Endocr. Regul. 2003,37(1):3-9.