Main content
Antimicrobial resistance (AMR) represents one of the defining public health challenges of our era. The most recent global estimates suggest that in 2021, 4.71 million deaths were associated with bacterial AMR, including 1.14 million deaths attributable to bacterial AMR. [1] AMR threatens to undermine decades of progress in medicine, from routine surgeries to cancer chemotherapy to neonatal care. The burden falls disproportionately on low- and middle-income countries (LMICs), where limited laboratory infrastructure, constrained formularies, and fragile healthcare systems compound the problem. [2] Yet the global response remains fragmented, oscillating between political declarations and innovation pipelines that often miss where antibiotics are actually used.
Into this landscape comes a timely State of the Art Review by Reza and colleagues in the BMJ, offering a comprehensive synthesis of AMR epidemiology, resistance mechanisms, prevention strategies, and emerging therapeutics. [2] The review deserves attention not merely for its scope but for its intellectual honesty about what current approaches can, and cannot, achieve.
The paper’s strengths lie in its systematic organisation of complex information. Informative tables provide an excellent overview of antibiotic classes, their mechanisms of action, and corresponding resistance pathways across key pathogens. Similarly, they summarise β-lactam/β-lactamase inhibitor combinations, and phase 3 trial results offer practical guidance on the expanding therapeutic armory against multidrug-resistant organisms. The review also makes the HIC–LMIC divide explicit: in all settings, empirical prescribing of essential antibiotics remains the cornerstone, while diagnostic-driven use of reserve agents represents a comparatively small fraction of use, even in high-income countries. [2]
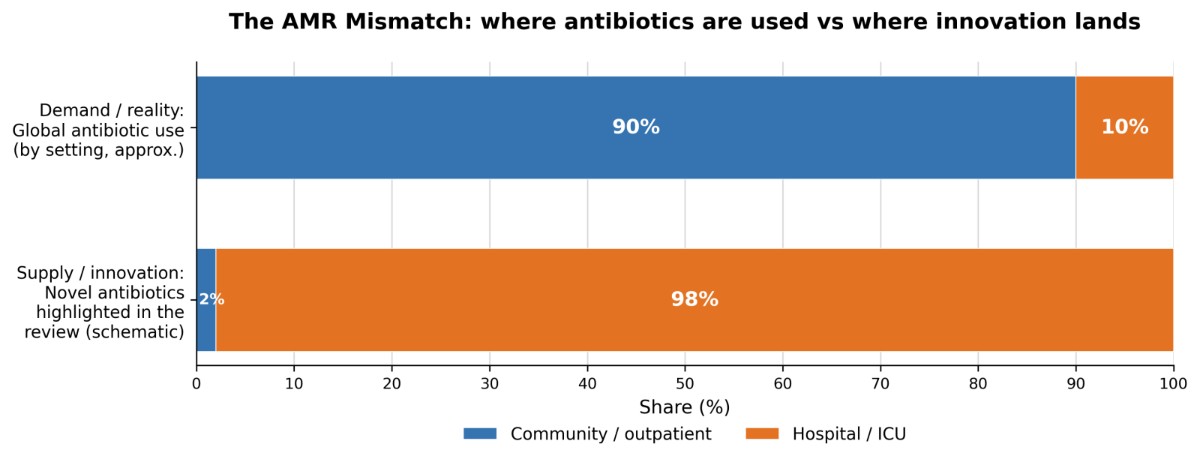
This is where the review becomes most sobering. It points out that policy attention and Research & Development (R&D) incentives often focus on specific “priority” resistance threats, while the antibiotics that dominate real-world consumption are overwhelmingly generic, essential agents (Figure 1). [2] In parallel, the United Nations General Assembly 2024 political declaration committed countries to reduce global deaths associated with bacterial antimicrobial resistance by 10% by 2030. [3] The declaration also reinforced antibiotic-use improvement goals aligned with the World Health Organization AWaRe (Access, Watch, Reserve) classification, including the indicator target that ≥70% of total antibiotic consumption should be Access-group antibiotics. [4] Reza and colleagues argue that, under the current global landscape, improvements in diagnostic capacity, prevention (water, sanitation and hygiene; infection prevention and control; vaccination), and antibiotic stewardship are unlikely on their own to be sufficient to achieve the intended mortality reductions. [2]
Herein lies the critical question the review raises but cannot fully answer. If better diagnostics remain inaccessible where most antibiotics are prescribed, if stewardship programmes struggle without laboratory support, and if prevention gains are structurally limited by infrastructure, then what constitutes a realistic strategy?
The uncomfortable truth may be that AMR cannot be “solved” through biomedical innovation alone. The problem is fundamentally socioeconomic: poverty-related determinants (crowding, limited WASH, malnutrition, delayed access to care) increasing infection incidence, health systems forcing empirical prescribing, and markets failing to sustain a vast range of antibiotic development. [5,6] Until we address why people need antibiotics, and why they use antibiotics, including use of antibiotics when they are not medically necessary, even the most advanced agents will remain technically exquisite but structurally misaligned. Cefiderocol, for example, is a genuine pharmacological innovation, a “Trojan horse” siderophore cephalosporin designed for highly resistant Gram-negatives, but it is also a high-income, high-control solution: expensive, tightly stewarded, and relevant to a narrow slice of patients. It cannot correct the dominant global drivers of resistance, high infection incidence, weak prevention infrastructure, and high-volume empirical use (and misuse) of first-line antibiotics in settings where diagnostics and regulatory control are limited.
Finally, surveillance illustrates the same mismatch: global systems such as WHO GLASS (the Global Antimicrobial Resistance and Use Surveillance System) are indispensable, but coverage and data completeness remain uneven, especially where burden is highest. [2,7] If measurement itself is fragile, “stewardship” becomes an aspiration rather than an actionable feedback loop.
Reza and colleagues have provided an invaluable resource. The challenge now is to read it not as a catalogue of progress, but as a call to rebalance our AMR strategy: to keep innovation moving, but judge success by what matters globally:
- fewer infections via water, sanitation and hygiene, infection prevention and control, and vaccination;
- affordable access to effective first-line therapy; and
- surveillance systems strong enough to turn stewardship from aspiration into feedback-driven practice.
Authors (all contributed equally to the article):
- Thomas Hänscheid, Universidade de Lisboa, Faculdade de Medicina, Instituto de Microbiologia; Center for Tropical Medicine and Travel Medicine, Department of Infectious Diseases, Amsterdam Infection & Immunity, Amsterdam Public Health – Global Health, Amsterdam UMC, Netherlands
- e-mail: t.hanscheid@medicina.ulisboa.pt
- João Carrasco, Faculdade de Medicina da Universidade de Lisboa, Instituto de Microbiologia, Lisboa, Portugal
- Inês Pato, Faculdade de Medicina da Universidade de Lisboa, Instituto de Microbiologia, Lisboa, Portugal
References:
- GBD 2021 Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024 Sep 28;404(10459):1199–1226. doi: 10.1016/S0140-6736(24)01867-1.
- Reza N, Dubey V, Sharland M, Hope W. Antimicrobial use and resistance. BMJ. 2025;391:e082681. doi:10.1136/bmj-2024-082681.
- United Nations. General Assembly adopts political declaration on antimicrobial resistance, demanding immediate action for safeguarding ability to treat disease, enhance food security. Press Release GA/12642 [Internet]. New York: United Nations; 2024 Oct 7 [cited 2026 Feb 6]. Available from: https://press.un.org/en/2024/ga12642.doc.htm
- World Health Organization. Indicator metadata: Target ≥70% of total antibiotic use being Access group antibiotics (AWaRe) [Internet]. Geneva: World Health Organization; (no date) [cited 2026 Feb 6]. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/5767
- O’Neill J. Tackling drug-resistant infections globally: final report and recommendations [Internet]. Review on Antimicrobial Resistance; 2016 [cited 2026 Feb 6]. Available from: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf
- World Bank. Drug-resistant infections: a threat to our economic future [Internet]. Washington (DC): World Bank; 2017 [cited 2026 Feb 6]. Available from: https://documents1.worldbank.org/curated/en/323311493396993758/pdf/final-report.pdf
- World Health Organization. Global antimicrobial resistance and use surveillance system (GLASS) report: 2022 [Internet]. Geneva: World Health Organization; 2022 [cited 2026 Feb 6]. Available from: https://www.who.int/publications/i/item/9789240062702