Main content
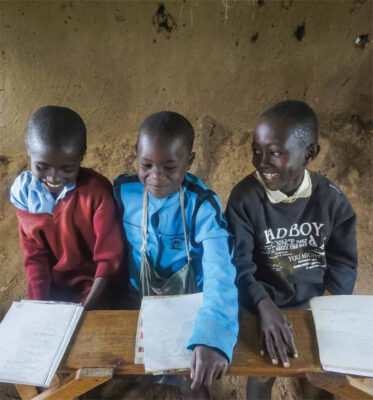
International Child Health Working Group Ouwehands Dierenpark, Rhenen – 11 March, 2016 Care for the refugee-child
In March this year, over 150 professionals with various backgrounds gathered at the annual congress of the International Child Health Working Group. Not only paediatricians, but also doctors in international health and tropical medicine (AIGTs), nurses, general practitioners, psychologists, policy makers, legal experts and volunteers found their way to ‘Ouwehands Dierenpark’ for this congress on refugee children.
Besides medical topics like haemoglobinopathies and tuberculosis screening, attention was given to the boat journeys that many refugees from Syria make to Europe. The Syrian paediatrician Dr Mohammed Ahmad shared his own experiences from living in the Dutch refugee camp Heumensoord as a medical professional.
Darren Cornish, general practitioner at the medical centre in Ter Apel refugee camp, gave an impassioned talk about his work with the refugees. He pointed out the need for more information about the whole process of logistics when arriving in the Netherlands. On this topic, regulations concerning health insurance appeared to be confusing and were further clarified by Christaan Rademaker, contract manager at the insurance company Menzis.
One of the main problems in caring for refugee children appears to be the lack of continuity. More than 90% of the children are treated in primary care, but diagnosis may be missed because of the many different health care workers involved. For example, during weekends in the refugee camp, triage is done by Red Cross staff, who are supervised by a doctor or nurse. Only after consultation by phone, can the patient be referred to a health centre nearby. In practice, this process appears to be time-consuming and inefficient. In hospital care as well, there are gaps in continuity due to the many relocations of refugees, leading to problems with transfer of medical information.
After the lunch break in the zoo, the congress program continued with a focus on care for mother and child. Jamilah Sherally (AIGT in training) discussed the option of adding a short internship in asylum centres to the education of the AIGT and using their dedication and skills in providing care for children and pregnant women in primary care. On the same topic, Peggy van der Lans, gynaecologist, pointed out the many issues around the vulnerable group of pregnant refugees, who deliver around 600 babies annually in the Netherlands. At present, maternal mortality has a risk ratio of 10, and it is likely that problems for mother and child continue after the delivery. Stakeholders like GGD-Ghor, Menzis MCA, GCA, COA, the Dutch Society of Midwives (KNOV) and the Dutch society of gynaecologists and obstetricians (NVOG) have developed a multidisciplinary guideline for the provision of care for these women.² This guideline is a good example of collaboration on care for asylum seekers, but its implementation must be improved.
Irma Hein, child psychiatrist at De Bascule in Amsterdam, then gave a presentation on psychotrauma. The incidence of psychopathology in refugee children is more than 25%, and 30%-70% have some symptoms. Moreover, 13%-25% of refugee parents suffer from post-traumatic stress disorder (PTSD) or depression with all its consequences for their children, including child abuse. The many underage refugees travelling alone (AMVs) with psychopathology have only the general practitioner to turn to after they turn 18. These refugees are particularly at risk of disappearing into the illegal circuit if they are denied legal status. There is an abundant although fragmented availability of preventive psychosocial aid programs, but they are mainly aimed at refugees in AZCs. The use of a good evidence based screening method like CRIES-13 is considered necessary. However, not many treatment methods are evidence based and it is still not clear when it is best to start treatment.
Maria van de Muijsenberg, general practitioner at Pharos, focused on the access to care and health insurance arrangements for the undocumented, illegal refugee child without a permit to stay. They often live with friends and family or on the street and lead an invisible life without much perspective. In this group reproductive health and behavioural or somatization issues often become problematic.³
Going on to discuss legal matters, Karin Kloosterboer (UNICEF Netherlands), explained that the situation with regard to children’s rights for the refugee child does not correspond in practice with the rules agreed upon. The many relocations with all the attendant consequences concerning social, emotional, educational, and medical issues as well as the group denied status after litigation deserve more attention.
The congress ended with a lively debate about this last topic, in which all the earlier speakers participated. The day was summarized by Albertine Baauw (paediatrician), who highlighted three main issues:
- The frequent relocations of refugees are harmful as they impede continuous delivery of healthcare and increase the risks of mental distress and developmental problems in children.
- Children of traumatized parents and those travelling alone are at high risk of psychosocial problems, which often only become clear after settling in the community or in illegality.
- There is an urgent need for early detection, valid screening, and evidence-based psycho-social interventions for this group.
All participants firmly agreed on the need to improve care for refugee children and pleaded for better collaboration between all parties involved, in order to optimize the care for this highly vulnerable group of children.

References
- www.RZAsielzoekers.nl
- www.knov.nl/vakkennis-en-wetenschap/tekstpagina/535/zorg-voor-zwangere-asielzoekers
- www.zorginstituutnederland.nl/verzekering/onverzekerbare+vreemdelingen.
Via www.ilegaalkind.nl, www.defenceforchildren.nl, www.stichtinglos.nl