Main content
Introduction
Malaria is not only a devastating disease in many tropical countries, it may also run a complicated course with significant morbidity and even fatalities in non-immune travellers. Most general hospitals in non-endemic countries have limited experience with malaria due to the relatively small number of malaria cases seen in returning travellers. This lack of experience may lead to a substantial delay in making an accurate diagnosis and timely treatment of malaria. This review provides a brief overview of imported malaria in the Netherlands and its changing landscape in terms of epidemiology, diagnosis, treatment and prevention.
Although the prevalence of malaria is declining worldwide, it is still a devastating disease in many tropical and sub-tropical areas. According to the World Malaria Report 2015 of the World Health Organisation (WHO), the estimated death toll of malaria worldwide approximated 438,000 deaths in 2014, most of them occurring in children under the age of five and pregnant women in sub-Sahara Africa.[1] Malaria may also occur in non-endemic countries as an imported disease, but clinical manifestation, disease course, and access to adequate diagnostic and treatment facilities may differ substantially from malaria endemic countries.
Epidemiology of imported malaria: declining incidence and changing traveller risk profile
Compared to malaria endemic countries, the prevalence of malaria in travellers in the Netherlands is very low, and a significant decrease of incidence has been observed over the past two decades (Figure 1), stabilizing at a plateau phase with a yearly 200 to 300 new cases. Plasmodium falciparum remains the most prevalent cause of malaria in travellers accounting for approximately 75% of the cases in the Netherlands, whereas P. vivax accounts for approximately 20% of the cases and the other Plasmodium species, P. ovale, P. malariae and the zoonotic monkey malaria P. knowlesi, occur relatively infrequently. The majority of P. falciparum infections in travellers are acquired in sub-Saharan Africa, whereas P. vivax infections in travellers are usually acquired in South-East Asia. In contrast to malaria endemic areas, the clinical picture of imported malaria in the Netherlands is dominated by its occurrence in adults with a clear preponderance for males. Even though effective drugs are available for chemoprophylaxis of malaria and an increasing number of travellers visit malaria-endemic regions, unprotected travellers increasingly outnumber travellers who are prescribed malaria chemoprophylaxis.[2] The contradictory observed decline in incidence of imported malaria in the Netherlands over the past decade was therefore linked to a decreased transmission risk of malaria at the target destination of the travellers. The influx of large numbers of refugees into the Netherlands may also influence the statistics of imported malaria. For example, the observed rise in the number of imported malaria cases in 2014 and 2015 was for the bigger part caused by an increased number of P. vivax cases diagnosed in Eritrean refugees.
Additionally, interesting changes have been observed in the travel profile of patients with imported malaria. Where in the past decades cases were almost exclusively seen in non-immune tourists, nowadays Visiting Friends and Relatives (VFRs) dominate the risk profile of imported malaria. VFRs are defined as immigrants, ethnically and racially distinct from the country of residence, who return to their homeland to Visit Friends and/or Relatives. Of note is that the VFR can be either an immigrant who was born in the destination country (‘immigrant VFR’) or someone not born in the destination country but with close ties, such as an immigrant’s child or other close family member (‘traveller VFR’). In general, VFRs seek far less pre-travel health advice than tourists or business travellers, frequently associated with insufficient awareness of the importance of health advice for travel, with the high costs of both consultation and personal protective measures, and with misconceptions about their own presumed immunity towards malaria combined with longer duration of exposure to malaria. VFRs are therefore at risk of contracting malaria again after visiting their homeland because their presumed immunity wanes in the absence of repeated exposure as is the case during their stay in The Netherlands. Even though the disease generally runs a less fulminant course as compared to naïve patients, cases of severe malaria and even fatal disease have also been described in VFRs. Known risk factors for severe malaria in travellers are non-use or inappropriate use of chemoprophylaxis, older age, delay in seeking care or diagnosis, incorrect treatment and non-immunity.[3]
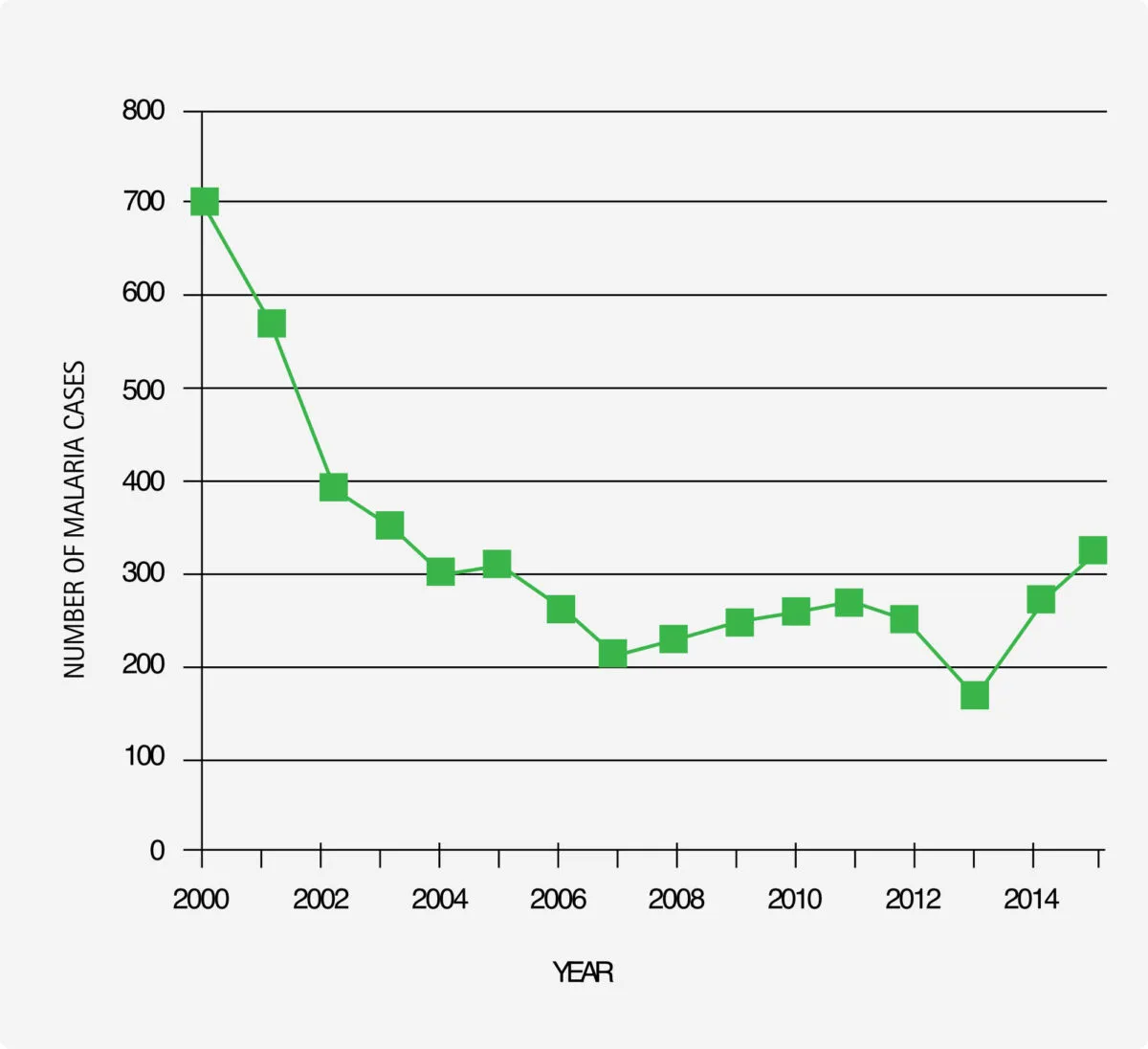
Source of data: Infectious Diseases Bulletin, National Institute for Public Health and the Environment, RIVM, Bilthoven, the Netherlands.
Diagnosis of imported malaria: the advance of rapid diagnostic tests for malaria
As malaria cannot be diagnosed on clinical grounds, tests are always required to make a proper diagnosis. Most standard blood parameters are non-specific for malaria, but thrombocytopenia, anaemia and elevated plasma LDH levels are frequently seen in malaria patients. In addition, increased plasma lactate was shown to be a useful predictor for disease severity in P. falciparum malaria.[4] Microscopic examination of thin and thick blood smears for malaria parasites is still considered the gold standard but increasingly rapid diagnostic tests (RDTs) are used as initial screening method. However, there are a number of important drawbacks to consider with the use of RDTs to diagnose malaria. First, RDTs may result in false-negative results in a substantial number of non-falciparum Plasmodium infections (including P. knowlesi) or in low-grade P. falciparum infections. Second, a positive RDT test result should be confirmed to exclude a false-positive test result, but also to determine the causative Plasmodium species and to determine the parasite load in order to assess disease severity. Third, false-negative RDT results may occur in certain genetic polymorphisms of Histidine Rich Protein 2 (HRP-2) variants geographically confined to the Asia-Pacific region and in P. falciparum isolates from South America lacking HRP-2. In addition, in some RDTs, false-negative test results may occur at high P. falciparum loads due to a so-called prozone effect, defined as false-negative or false-low results in immunological reactions due to an excess of either antigens or antibodies. Finally, it should also be borne in mind that reactivity of the P. falciparum-specific protein HRP-2 band together with reactivity of the pan-plasmodium LDH or aldolase band is not only indicative of a monoparasitic P. falciparum infection but may also be a feature of a mixed Plasmodium infection (for reference, about 0.7% of all Plasmodium infections in The Netherlands were attributable to mixtures of species, mostly involving P. falciparum).
In addition to RDTs and microscopic examination of stained blood smears, several other sensitive methods are available in health care centres specialized in tropical diseases, such as Quantitative Buffy Coat (QBC) analysis and real-time quantitative PCR. These techniques are not widely used, as QBC analysis requires well-trained technicians and a costly fluorescent microscope and PCR is still a relatively time-consuming method.
Treatment of imported malaria: the advance of artemisinin-based treatment regimens
In its essence, the treatment of P. falciparum malaria and non-P. falciparum malaria does not differ between endemic and non-endemic countries. In the past decade, the artemisinin-combination therapy (ACT) acquired a dominant role in the treatment of uncomplicated (chloroquine resistant) P. falciparum malaria, whereas chloroquine is reserved for the treatment of sensitive non-P. falciparum strains. Also, in both endemic and non-endemic countries, intravenous artesunate replaced intravenous quinine as the drug of choice for the treatment of severe malaria [6,7] and contributed significantly to an increased survival of severe malaria cases, with up to 33% relative reduction of mortality in endemic regions. Post-marketing surveillance studies revealed that a delayed haemolysis may occur 2-4 weeks after artesunate treatment of severe malaria. Risk factors include hyperparasitemia and young age. All patients treated with parenteral artesunate should therefore be followed up for at least four weeks after artesunate to detect signs of haemolysis and to allow appropriate symptomatic treatment.[8]
The differences in mortality of severe P. falciparum malaria in endemic and non-endemic countries like The Netherlands are conceivably due to differences in availability of proper antimalarials like artesunate and access to supportive or intensive care facilities. In the Netherlands, the mortality of imported severe P. falciparum malaria is extremely low because of our well-organized health care system and the availability of artesunate and supportive care measures like mechanical ventilation, renal replacement therapy, vasopressors, fluid resuscitation, restoration of coagulation disorders, broad-spectrum antibiotics, blood transfusion, and sometimes blood exchange transfusion or selective erythrocytapheresis.[7] After the introduction of artesunate treatment for severe malaria almost a decade ago, the additional benefit of exchange transfusion in terms of parasite clearance was shown to be negligible,[6] and therefore exchange transfusion has been largely abandoned.
Prevention of imported malaria
Since malaria in travellers can be a fulminant and fatal disease, travellers to malaria endemic areas are advised to adhere to chemoprophylaxis for malaria. Although none of the prophylactic regimens offer 100% protection against malaria (inadequate efficacy especially against non-P. falciparum malaria), it does protect against the development of severe P. falciparum malaria if taken meticulously.[10] However, the perceived side effects of malaria chemoprophylaxis often cause the traveller to refrain from malaria chemoprophylactic drugs. As a kind of compromise, travel health authorities in the German speaking European countries advise stand-by treatment for travellers to areas with a low prevalence of malaria, i.e. a course of artemether-lumefantrine or atovaquone-proguanil to be used in case malaria is suspected. The results of standby treatment look promising. Active surveillance did not find an increase in the number of malaria cases after implementation of this preventive policy in the German-speaking countries. The Dutch Coordinating Centre for Health Advice is currently considering this policy for implementation in the Netherlands.
Concluding remarks
In this review, several aspects of imported malaria have been discussed. Due to a decreased transmission risk, a decreasing number of malaria cases have been observed in the past decade, especially in non-immune Dutch tourists. Refugees from malaria endemic regions may cause a resurgence of imported malaria cases in the Netherlands. Diagnostic tests for malaria increasingly rely on rapid diagnostic tests for initial screening, but their use is associated with several important limitations. Intravenous artesunate has replaced quinine as the treatment of choice for imported severe malaria. Given the potentially fatal course in non-immune individuals, malaria chemoprophylaxis is advised for travellers entering a high-risk malaria endemic country, but this advice is being increasingly ignored due to the presumed side effects. Stand-by treatment may provide a valuable alternative policy for prevention in low- to medium-risk malaria regions.
References
- World Health Organisation Malaria report 2015. WHO Press, Geneva, Switzerland.
- van Rijckevorsel GG, Sonder GJ, Geskus RB, Wetsteyn JC, Ligthelm RJ, Visser LG, Keuter M, van Genderen PJJ, van den Hoek A. Declining incidence of imported malaria in the Netherlands, 2000-2007. Malar J. 2010; 9:300.
- Lüthi B, Schlagenhauf P. Risk factors associated with malaria deaths in travellers: a literature review. Travel Med Infect Dis. 2015; 13:48-60.
- van Genderen PJJ, van der Meer IM, Consten J, Petit PL, van Gool T, Overbosch D. Evaluation of plasma lactate as a parameter for disease severity on admission in travelers with Plasmodium falciparum malaria. J Travel Med. 2005; 12:261-4.
- Maltha J, Gillet P, Jacobs J. Malaria rapid diagnostic tests in travel medicine. Clin Microbiol Infect. 2013;19:408-15.
- Kreeftmeijer-Vegter AR, de Mendonça Melo M, de Vries PJ, Koelewijn R, van Hellemond JJ, van Genderen PJJ. Manual blood exchange transfusion does not significantly contribute to parasite clearance in artesunate-treated individuals with imported severe Plasmodium falciparum malaria. Malar J. 2013;12:115.
- Kreeftmeijer-Vegter AR, van Genderen PJJ, Visser LG, Bierman WF, Clerinx J, van Veldhuizen CK, de Vries PJ. Treatment outcome of intravenous artesunate in patients with severe malaria in the Netherlands and Belgium. Malar J. 2012;11:102
- Rolling T, Agbenyega T, Krishna S, Kremsner PG, Cramer JP. Delayed haemolysis after artesunate treatment of severe malaria – review of the literature and perspective. Travel Med Infect Dis. 2015;13:143-9.
- Askling HH, Bruneel F, Burchard G, Castelli F, Chiodini PL, Grobusch MP, Lopez-Vélez R, Paul M, Petersen E, Popescu C, Ramharter M, Schlagenhauf P & European Society for Clinical Microbiology and Infectious Diseases Study Group on Clinical Parasitology. Management of imported malaria in Europe. Malar J. 2012;11:328.
- Vliegenthart-Jongbloed K, de Mendonça Melo M, van Wolfswinkel ME, Koelewijn R, van Hellemond JJ, van Genderen PJJ. Severity of imported malaria: protective effect of taking malaria chemoprophylaxis. Malar J. 2013;12:265.